
Drug-to-drug interaction. New evidences about Morphine.
The lead interventional cardiologist in Cardiovascular and Thoracic Department of Careggi Hospital in Florence (Italy), Guido Parodi, wrote an interesting article on medest118.com about drug-to-drug interaction.
Recent literature shows a growing risk of mortality in STEMI patients treated with morphine. Guido, in his article, said “despite the complete absence of rigorous studies designed to assess the impact of morphine administration in patients with AMI, clinical practice guidelines for the management of patients with STEMI strongly recommend the use of morphine for analgesia.”
2015 CRUSADE registry analysis has highlighted that patients treated with morphine had higher adjusted risk of death than patients not treated with it even after using a propensity score matching method.
An additional explanation of the negative impact of morphine on AMI outcome can be related to drug interactions.
Morphine inhibits gastric emptying, delaying absorption and so decreasing peak plasma levels of orally administered drugs in general and antiplatelet agents; this is a biologically cause effect relation.

The same author in 2015 demonstrated, in another study called “Morphine is associated with a delayed activity of oral antiplatelet agents in patients with ST elevation acute myocardial infarctionundergoing primary PCI”, that the negative impact of morphine on platelet inhibition was not only limited to patients who vomited (patients with vomiting were excluded), but morphine-treated patients clearly showed higher residual platelet reactivity compared with patients who did not receive morphine.
Professor Montalescot, one of the lead authors of the ATLANTIC Trial, noted:“Co-administration of morphine in the ambulance may have delayed ticagrelor’s onset of action. To what extent this interaction may have affected our results remains unknown at this stage.”
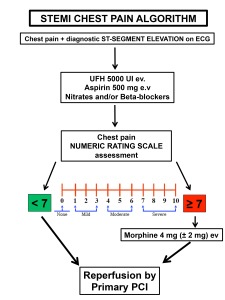
In conclusion the author said that morphine administration has to be reserved just for level of pain equal or superior to 7 on the base of a numerical rating scale (NRS) related value. In case of lower chest pain intensity (NRS ≤ 7) alternative strategies should be persecuted, for example paracetamol (1g) or aspirin (≥300 mg) can be alternative choices to reduce chest pain as is well demonstrated in literature.
Full article here.