

Bipolar disorders: mood stabilisers or flattening?
When indicating the goal of therapy for recurring mood disorders, in particular major bipolar disorders, the term commonly used is ‘stabilisation’, i.e. mood-stabilising medication to indicate the therapeutic tool, or ‘mood-regulator’, i.e. mood-regulator
Mood instability on a straight line
These terms sound obnoxious to many, because they give the idea of forcing one’s mood and its facets towards a hypothetical flat line, intermediate between depression and excitement.
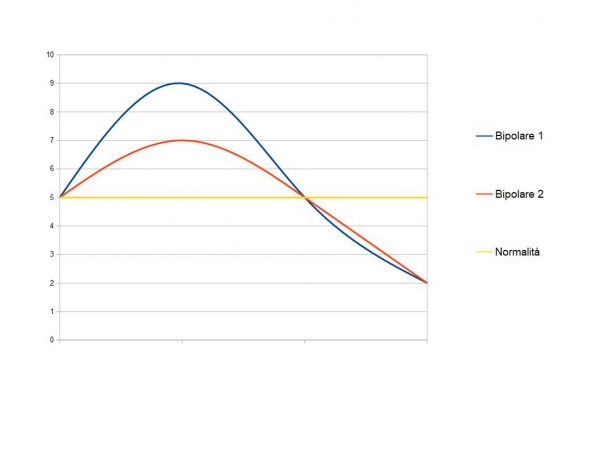
In the most widespread graphical representation, mood disorders are represented as curves up or down in relation to a ‘zero’ line, where the amplitude indicates the severity of the symptoms, the width the duration, and the direction the mood ‘pole’.
In this graphic by the way, the mixed state already does not have its own linear translation (it is represented with vertical bars) and the further a point is from the zero line, the more it tends to be followed by a true phase if it continues over time. This is relative, however.
There are, for example, stable lines of depression and also ‘stable’ mixed states, whereas a stable ‘line’ of mania is less likely.
Flexibility and rigidity
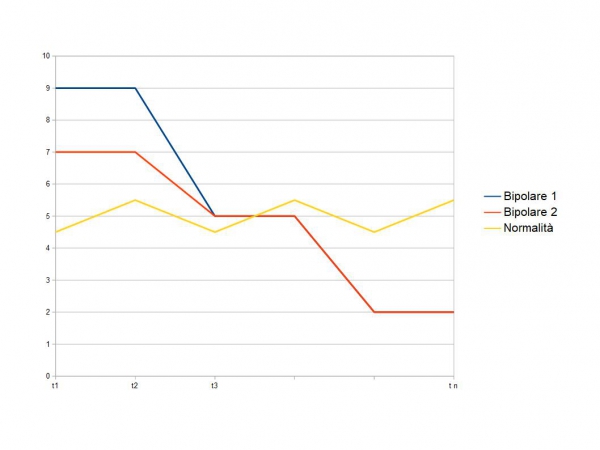
The line, however, gives the idea of series of equal points.
This does not resemble the physiology of mood, but rather resembles the rigidity of the phases of disorders.
One can be rigid depressed or rigid excited and in this case one has to imagine normality as an undulating line, irregularly and in a manner dependent on external stresses, just as it can be a liquid medium, which undulates and adapts, rises and falls in level, has internal currents and ripples.
Pathology begins when the liquid becomes solid and its ability to adapt and change is reduced.
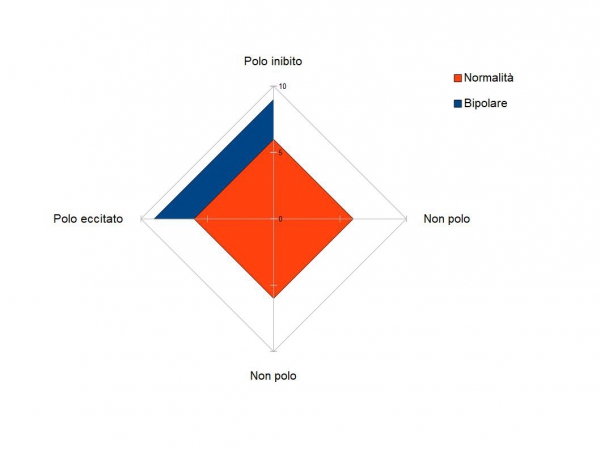
This rigidity recalls other concepts common to the various phases of bipolar disorder: synchronisation (the various functions are all shifted towards the same pole, excited or inhibited) and polarisation (a function is expressed in a deviated manner towards one pole, excited or inhibited).
In these terms, there is more similarity between depression and mania than there is between normality and either phase, albeit of opposite polarity.
The rigidity of the mood, which does not change with external stresses but persists in a ‘polar’ set-up, is flat, it is a crushing against the floor or against the ceiling.
Flexibility at the centre, rigidity at the poles.
It is also known that in bipolar disorder the mood is not stable and is subject to abrupt ‘virages’, and in the excited phases brief depressive virages, mostly agitated, are not uncommon.
The viraggies could be represented as a transition, but not under or over a line, but to the right or left of the same plane of crushing, of polarisation.
Probably this plane, this time for better to say, on which the mood flows from one pole to the other, is different for depressive illnesses (which have only one pole), and bipolar illnesses.
Why we talk about mood stabilisers
As far as treatment is concerned, the word ‘stabiliser’ was invented to indicate what should happen, but applied to medicines that in reality are still studied as acute phase anti-exciters (anti-manic).
There may in fact be medicines that are able to cure mania and prevent manic relapses, without being able to prevent depressive relapses.
There is, for some medicines, a certain continuity between preventing one phase and the others when they are part of a cycle: blocking the beginning of the cycle prevents the rest of the cycle.
The desired result with a mood stabiliser is to bring a person’s mood and related functions back to a stable pliability and ripple.
Some patients, on the other hand, complain of a ‘flat’ stability, a kind of excessive anti-excitatory effect, which does not reproduce a dynamic and undulating bottom, but a squashed and firm one.
In particular, people accustomed to a direct relationship with sources of humoral stimulation (e.g. drugs) are very sensitive to this ‘squashed-down’ tone.
Posthumous stabilisation
A final consideration concerns the posthumous stabilisation after spontaneous phases of mania, after the resolution of the depression that may have followed or after phases of exposure to euphoric substances.
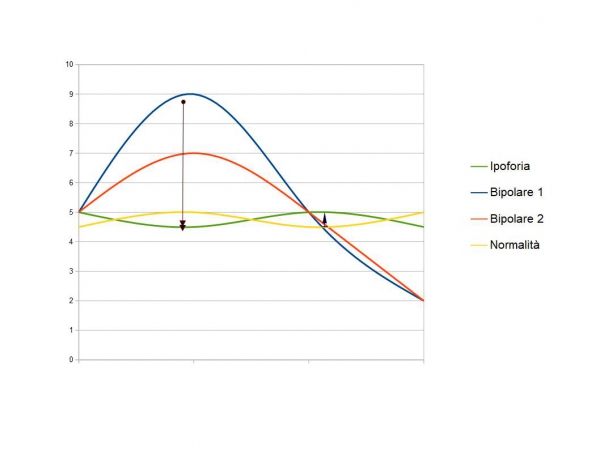
The range of normality, which provides for a certain variability of mood qualities within a certain range of intensity without polarisation, is restricted in these cases.
The person may be stable, inoffensive, functional, but he or she does not show humoral liveliness and may experience this condition as ‘hypohoric’, i.e. impaired, for better or worse.
Obviously, the sensitivity of the person who has experienced peaks of euphoria is much greater with regard to the lack of euphoria than with a mildly depressed person: technically, the mildly depressed person is more dull than the hypophoric, but the hypophoric person experiences a greater difference, because his reference is mania or hypomania.
Moreover, whereas the ‘normal’ depressive retains the capacity for counter-drive, and thus tends to do something to return at least to the level of normality tending upwards, the hypophoric feels squeezed downwards, and is thus still polarised, despite being quantitatively ‘normal’.
His ‘threshold’ of normality has risen, and he does not feel normal unless he is overstimulated.
Apparently he is normal-depressed, he might give the idea that he is permanently switched off, instead he simply carbonizes less, but is still inflammable.
Unfortunately, if he has to be inflamed in order to remain more inflamed, this damage worsens, so the point is to improve his carburation, and not to seek ever newer and more intense ways of reproducing transient flare-ups.
Read Also
Emergency Live Even More…Live: Download The New Free App Of Your Newspaper For IOS And Android
Medications For Bipolar Disorder: Antidepressants And The Risk Of Manic Phases
Mood Disorders: What They Are And What Problems They Cause
Antidepressant Drugs: What They Are, What They Are For And What Types Exist
Everything You Need To Know About Bipolar Disorder
Drugs To Treat Bipolar Disorder
What Triggers Bipolar Disorder? What Are The Causes And What Are The Symptoms?
Depression, Symptoms And Treatment
Narcissistic Personality Disorder: Identifying, Diagnosing And Treating A Narcissist
Intermittent Explosive Disorder (IED): What It Is And How To Treat It
Bipolar Disorder (Bipolarism): Symptoms And Treatment
Psychosomatic Dermatitis: Symptoms And Treatment
Intranasal Esketamine, The New Drug Approved For Resistant Depression

What You Need To Know About Substance Use Disorder
Seasonal Depression Can Happen In Spring: Here’s Why And How To Cope
Major Depressive Disorder: Clinical Features
Intranasal Ketamine For The Treatment Of Patients With Acute Pain In ED
The Use Of Ketamine In Pre-Hospital Setting – VIDEO
Ketamine May Be Emergency Deterrent For People At Risk Of Suicide
What Is Ketamine? Effects, Uses And Dangers Of An Anaesthetic Drug That Is Likely To Be Abused
6 Ways To Emotionally Support Someone With Depression
Defusing Among First Responders: How To Manage The Sense Of Guilt?
Paranoid Personality Disorder: General Framework
The Developmental Trajectories Of Paranoid Personality Disorder (PDD)
Reactive Depression: What It Is, Symptoms And Treatments For Situational Depression
In Daily Life: Dealing With The Paranoid
Amaxophobia, How To Overcome The Fear Of Driving?
Hesitation When Driving: We Talk About Amaxophobia, The Fear Of Driving
Emotional Abuse, Gaslighting: What It Is And How To Stop It
Facebook, Social Media Addiction And Narcissistic Personality Traits
Social And Exclusion Phobia: What Is FOMO (Fear Of Missing Out)?
Paranoid Personality Disorder: Symptoms, Diagnosis And Treatment
Gaslighting: What Is It And How To Recognise It?
Nomophobia, An Unrecognised Mental Disorder: Smartphone Addiction
The Panic Attack And Its Characteristics
Psychosis Is Not Psychopathy: Differences In Symptoms, Diagnosis And Treatment
Metropolitan Police Launches A Video Campaign To Raise Awareness Of Domestic Abuse
Amaxophobia, The Fear Of Driving
Fear Of Flying (Aero-Phobia-Avio-Phobia): What Causes It And What It Is Caused By
Metropolitan Police Launches A Video Campaign To Raise Awareness Of Domestic Abuse
World Women’s Day Must Face Some Disturbing Reality. First Of All, Sexual Abuse In Pacific Regions
Child Abuse And Maltreatment: How To Diagnose, How To Intervene
Child Abuse: What It Is, How To Recognise It And How To Intervene. Overview Of Child Maltreatment
Does Your Child Suffer From Autism? The First Signs To Understand Him And How To Deal With Him
Rescuer Safety: Rates Of PTSD (Post-Traumatic Stress Disorder) In Firefighters
PTSD Alone Didn’t Increase Heart Disease Risk In Veterans With Post-Traumatic Stress Disorder
Post-Traumatic Stress Disorder: Definition, Symptoms, Diagnosis And Treatment
PTSD: First responders find themselves into Daniel artworks
Dealing With PTSD After A Terroristic Attack: How To Treat A Post Traumatic Stress Disorder?
Surviving death – A doctor revived after attempting suicide
Higher risk of stroke for veterans with mental health disorders
Stress And Sympathy: What Link?
Pathological Anxiety And Panic Attacks: A Common Disorder
Panic Attack Patient: How To Manage Panic Attacks?
Panic Attack: What It Is And What The Symptoms Are
Rescuing A Patient With Mental Health Problems: The ALGEE Protocol
Eating Disorders: The Correlation Between Stress And Obesity
Can Stress Cause A Peptic Ulcer?
The Importance Of Supervision For Social And Health Workers
Stress Factors For The Emergency Nursing Team And Coping Strategies
Italy, The Socio-Cultural Importance Of Voluntary Health And Social Work
Anxiety, When Does A Normal Reaction To Stress Become Pathological?
Physical And Mental Health: What Are Stress-Related Problems?
Narcissistic Personality Disorder: Identifying, Diagnosing And Treating A Narcissist