

Patient's state of consciousness: the Glasgow Coma Scale (GCS)
The Glasgow Coma Scale (GCS) is used to describe the level of consciousness in an individual. It is often used to gauge the severity of an acute brain injury due to trauma or medical cause
The test is simple, reliable, and correlates well with outcomes following brain injury.
It is composed of 3 domains which are assessed separately and given numerical scores.
The sum of these scores is the Glasgow Coma Score (GCS)
The three areas are
- Eye Opening,
- Verbal Response, and
- Motor Activity.
EYE-OPENING (1-4 Points)
- Does not open eyes in response to anything.
- Opens eyes in response to painful stimuli.
- Opens eyes in response to voice.
- Opens eyes spontaneously.
VERBAL RESPONSE (1-5 Points)
- Makes no sounds.
- Incomprehensible sounds.
- Utters incoherent words.
- Confused, disoriented.
- Oriented, converses normally.
MOTOR ACTIVITY (1-6 Points)
- Makes no movements.
- Decerebrate (extensor) posture (an abnormal posture that can include rigidity, arms and legs held straight out, toes pointed downward, head and neck arched backward).
- Decorticate (flexor) posture (an abnormal posture that can include rigidity, clenched fists, legs held straight out, and arms bent inward toward the body with the wrists and fingers bend and held on the chest).
- Withdrawal from painful stimuli.
- Localizes to painful stimuli.
- Obeys commands.
EXAMPLE: So a patient who has scores of Eye = 3, Verbal = 4 and Motor = 5 is said to have a GCS of 12.
You would express this as a GCS 12 = E3, V4, M5.

There are some GCS scores that are significant and must be memorized:
3: The lowest possible GCS; this indicates a patient is wholly unresponsive.
8: The point of intubation; any patient with an 8 or lower is strongly considered for intubation, as they are unlikely to maintain a patent airway.
15: The highest GCS score; a patient who opens their eyes spontaneously, is oriented and alert, and obeys commands has a GCS of 15.
MODIFIERS:
Modifiers are used to eliminate misleading scores–it’s all about accuracy, especially as it pertains to outcomes. For example:
You can communicate that the patient is intubated with modifiers like V1t where it indicates that the patient makes no verbal sounds but it’s secondary to an (endotracheal) tube.
Other common modifiers are E1c where “c” stands for closed due to swelling or damage. Sometimes, the “1” is omitted, and instead of using V1t, you could just see Vt since, in that case, the 1 is seen as a redundancy.
GLASGOW COMA SCALE (GCS), PEDIATRIC CONSIDERATIONS:
A child’s reaction to his own health crisis will not be the same as an adult’s. Understanding commands and cooperating with them can be compromised due to pain or immaturity.
The GCS is not well validated in children and cannot–as a sole indicator–predict the need for airway interventions.
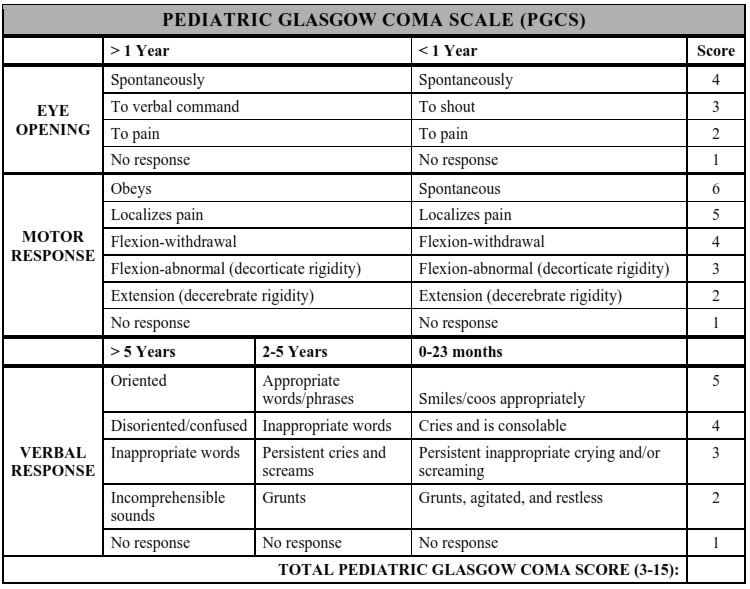
The best approach in considering intubation for childhood trauma is to assess for valid indications for intubation, such as a child who cannot maintain his/her airway (determined with phonation and swallowing, not just the gag reflex).
A separate Pediatric Glasgow Coma Scale was created because young children can be harder to assess for verbal and motor function as they may not have the ability to answer your questions or follow instructions adequately.
GCS in Plain English:
We are assessing responsiveness because being able to react to stimuli means the brain is working.
MEMORY TOOL: For GCS SCORING, Remember 1,2,3,4,5,6 (Three Questions and 3 Scores)
There are 3 questions: 1) Do his eyes respond? 2) Does he verbally respond? 3) Does he respond with his body?
There are 3 max points: 4) Eyes get a max of 4 points, 5) verbal gets 5 points, 6) motor gets 6 points.
So, 1, 2, 3, 4, 5, 6

Instead of writing GCS score to begin with, just start PRACTICING with using E4, S5, M6. Get in the habit of looking at a patient and judging his response. If he’s totally responsive, he’s E4, S5, M6. If he’s a little confused, like after a concussion, but his eyes open and he has purposeful movements, then you only have to take 1 from speech. So the confused guy is E4, S4, M6.
Use it like a checklist. Do his eyes open? If yes, then score a 4. If no, then score a 1. If “kinda,” then look at the criteria. Same with the other 2. Check yes or no or kinda. If “kinda” then check out that specific list and proceed.
DO HIS EYES OPEN? (Max 4) (Eyes are easy, you’re assessing eye AVPU)
No matter what I do, his eyes don’t open.
Eyes open when I inflict pain
Eyes open when I call his name
Eyes are normally open
IS HE TALKING CORRECTLY? (Max 5)
He’s not talking at all
He’s just making sounds
He’s saying words, but they don’t make sense
He’s talking, but he’s confused
He’s talking normally
IS HE ABLE TO MOVE HIS OWN BODY? (Max 6)
He’s not moving, no matter what I do.
If I apply pain, his body flexes away from his core. Extension.
If I apply pain, his body tightens towards his core. Flexion.
If I apply pain, his body tries to back away from the pain spot.
If I apply pain, he moves his hand to the pain spot.
He is moving on his own.
Read Also:
Emergency Live Even More…Live: Download The New Free App Of Your Newspaper For IOS And Android
Post-Arrest Temperature Management In Children
Cincinnati Prehospital Stroke Scale. Its Role In Emergency Department
How To Rapidly And Accurately Identify An Acute Stroke Patient In A Prehospital Setting?
Cerebral Haemorrhage, What Are The Suspicious Symptoms? Some Information For The Ordinary Citizen
ABC, ABCD And ABCDE Rule In Emergency Medicine: What The Rescuer Must Do
Rapid Blood-Pressure Lowering in Patients with Acute Intracerebral Hemorrhage
Tourniquet and intraosseous access: massive bleeding management
How to rapidly and accurately identify an acute stroke patient in a prehospital setting?
Glasgow Coma Scale (GCS): How Is A Score Assessed?
Pediatric Glasgow Coma Scale: Which GCS Indicators Change In The Paediatric Coma Scale